Engaging Gluteus Maximus and Minimizing Foot
and lower Leg Injuries.
Note: For information about the linkage between bare foot running and Engaging Gluteus maximus, see
Engage Gluteus maximus, Introduction.
It has certainly been established that lower limb injuries
can be minimized by
going bare-foot. (For example, bare-foot running is a proven plantar fasciitis treatment).
See quote:-
- "Where barefoot and shod populations co-exist, as in Haiti, injury rates of the
lower extremity are substantially higher in the shod population".(8)
Many of the bare-foot benefits can be achieved and maintained by incorporating a
short once weekly run or brisk walk on rough ground, and by learning and applying the healthy
type of walking/running that the pain will teach you - Yes, it is painful on the soles of the feet,
And yes, the pain does teach.
Let me share with you my experience of 3 months of bare foot running.
It is not always advisable to go bare-foot. If there is glass or snow
on the ground, it's better to have your feet comfortably and warmly shod!
As already discussed, this type of travel
involves engaging Gluteus maximus at "heel strike".
By now you will have experienced "Engaged Glute" walking that is one of the
things that bare-foot walking enhances. You will also have experienced that
the following joints are no longer at extremes of range of motion at foot landing:-
- The ankle no longer goes to the extreme of dorsi-flexion (toe still
high off the ground when the heel starts to weight bear).
- The knee no longer goes to the extreme of extension.
In summary, your full body weighting at foot strike is experienced on the mid foot
with the body more nearly over the foot rather than behind it and coming forward over
it. This is good running technique(17).
Let's take time to analyse what this means in terms of musculo-skeletal health
of the lower limb. We shall discuss the following:-
- Ankle Sprain Treatment
- Plantar fasciitis due to Flat Feet & Treatment
- Tibialis Posterialis Tendinosis (Another Flat Footed Syndrome).
- Shin Splints and Anterior Compartment Pressure Build up.
- Peri-Patella Pain and the "Q-Angle"
- Tensor Fascia Lata - Iliotibial Band (TFL-ITB)Strain and Trochanteric bursitis.
1 Ankle Sprain Treatments.
Bare feet are less likely to cause ankle
sprains(4). There are a number of reasons:
- The foot lands on its full surface and not just the
heal: that makes it a more stable platform.
- The sole of the foot gets a greater sensory input, which tends to trigger the
ballancing responses in the Gluteus maximus and foot and lower limb (see"Bare-foot Walking Exercise"
already discussed in this article).
- "...prior ankle injury [is] associated with delay of the gluteus maximus in
contributing to hip extension"(18)
- Engaged gluteus will help, because during one legged stance,
the gluteal muscle
is a hip abductor/lateral rotator muscle and will minimize the "hip adduction
with medial hip rotation" at heel strike that makes you vulnerable to ankle twist (see pictures
of Ankle Sprain Prevention below).
The Gluteus will minimize "hip adduction with medial rotation",
which is the directional susceptibility of movement associated with Ankle Sprain
Pictures of Ankle Sprains:
Diagram left: Hip adducted and femur medially rotated. Ankle twist occurs easily with this
directional susceptibility of movement.
Diagram Right: Hip not adducted and femur laterally rotated. The ankle is not
about to twist!
|
 |
 |
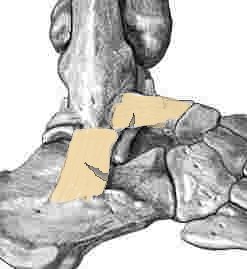
Pictures of Ankle Sprains
Diagram Left: Close up of Foot at moment of Ankle Sprain
Diagram Right: Close up of the Bones and Ligaments. The vertical ligament is the
Calcaneofibular ligament. The horizontal ligament is the Anterior Talofibular ligament
|
 |
 |

2. Plantar fasciitis due to Flat Feet.
Before we discuss the disease processes behind plantar fasciitis, we need to be able to recognise the
faulty posture-movement pattern that is the actual cause of plantar fasciitis:-
| The Faulty posture and movement pattern
that causes plantar fasciitis... |
...is hip medial
rotation (with or without hip adduction) accompanied by foot pronation (flat feet).
Don't be put off by the technical description.
The movement pattern is extremely easy to recognise! You could call it "knock knees".
You can see it in the lower picture to the right.
Diagram Right:
Sit to Stand Movement with Gluteus maximus engaged and foot arches fully formed.
Pictures, Normal Feet:-

|
Healthy Sit to Stand Movement:
 |
Diagram Right:
Sit to Stand Movement with the Gluteus maximus not engaged and the
foot arches collapsing into Foot pronation. The medial (inside arches)
of the foot are taking the weight. In plantar fasciitis, it is the ligaments on this side that
become injured due to increased loading.
Pictures, Flat Feet:- 

|
Knock Kneed Sit to Stand Movement:
 |
The Disease Process behind Plantar Fasciitis
|
In the runner, maximal shock wave jarring of the foot arch ligaments and muscles occurs just before "toe-off".
If "toe-off" is performed with the knee collapsing inwards and on a flat foot, then the shock wave jarring,
- and therefore the loading - is transmitted
through the medial (big toe) side of the foot arch. Combine this "lop-sided" jarring of the foot arch
with poor foot arch muscle strength (weak foot arch muscles are commonly associated with expensive
running shoes and custom orthotics), and you can understand why the ligaments and tendons
between the big toe and the heel are strained. The foot arch muscles respond to the pain of
this tendon and ligament damage by shortening into continuous spasm, so that even when you are sleeping, the
ligaments are under tension and not able to pull their partially torn ends together for healing to occur.
so that the night time punishment inflicted by those spasming muscles makes
plantar fasciitis treatment all the more slow and difficult.
Note: The size of shock wave jarring in the foot arch will be increased by poor "give" in the calf muscles.
So plantar fasciitis treatment requires that you also stretch and strengthen your calf muscles.
|
Diagram:
Just before "Toe-Off"
 |
Conclusion regarding Plantar Fasciitis Treatment:
To avoid plantar fasciitis, and similarly to provide an effective plantar fasciitis treatment,
you need to avoid "knock knees" during all stages of walking and running,
and work on the strength and competence of the foot arch muscles and calf muscles.
To avoid knock knees, your Gluteus maximus must engage at "foot fall" and during the sit to stand manoeuver.
3 Tibialis Posterialis Tendinosis
The Posterior tibial muscle contributes to the formation of the foot arch (see
diagram). The discussion under :"Plantar fasciitis treatment" (see above) regarding the faulty posture-movement
pattern of "hip adduction with medial rotation" can be applied equally to the posterior tibial muscle.
I would argue that the cause of Tibialis Posterialis Tendinosis is very similar to the cause of plantar fasciitis.
Certainly, both conditions are associated with flat feet, and are more painful after lying down, i.e. both conditions
have a muscle splinting component due to irritation at their tendinous attachments.
4. Shin Splints and Anterior Compartment Pressure Build up.
"Barefoot runners land mid-foot [as opposed to heel landing], and with a slightly
more plantar-flexed ankle".(4)
Gluteal contraction alone tends to do this too.
Mid foot landing (see pictures below) means that the anterior compartment muscles (at the front of the shin) do not have to work so hard.
When the
anterior shin muscles are not called upon to work hard, they are less likely
to develop "shin splints" and anterior compartment syndrome. (I have
certainly found this to be true for myself).
The heel landing of the shoed runner tends to be with a fully flexed ankle, and this means that the muscles inside the
anterior compartment (front of the shin) are being requested to contract maximally at their shortest length, where they are weakest.
Whereas with mid foot landing, the anterior compartment muscles are working at their mid-range,
where they are at their strongest. In addition, with mid-foot landing, they are not being
called upon to do a full range of movement,
nor are they being asked to be the prime stabilizers for a long period of time,
so that they are not working so hard.
Diagram 1: Westerner's heel strike. Note the dorsi-flexion.
Ball of toe still well above ground.
 |
Diagram 2: Westerner's foot at moment of Foot "Slam down". Lower leg is still
tilted backward, and the ankle is not in its strong middle position.
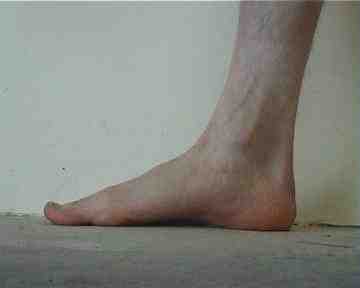 |
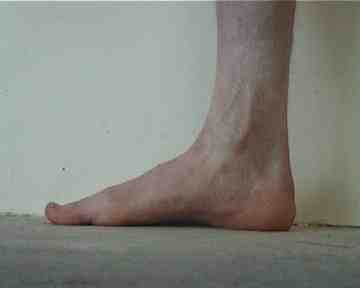
Diagram 3: Bushman's foot touchdown. Minimal dorsiflexion, and the ball of the toe is already
close to the ground.
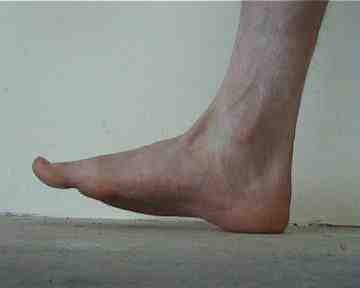 |
Diagram 4: Bushman's foot at the moment of Foot "Touchdown".
It doesn't "slam down", and the
ankle is in its strong middle position.
 |
The foot arch
forming muscles are comprised of:-
- The short muscles within the arch of the foot (there are four layers of them,
comprising 50 individually named muscle units!!!).
- The long muscles which are housed in the tibial posterior compartment (Tibialis
posterialis and the long flexors of the toes).
For the author's experience with mild posterior tibial tendinosis, refer to
the appendix to this article "Pain Free Running in Just Three Months!"
5. Peripatellar Pain and the "Q"-angle
"...peri-patellar pain [is] attributed to excessive shock loading of
the limbs. When running barefoot on
hard surfaces, the runner compensates for the lack of cushioning underfoot by
plantar-flexing the foot at contact [probably better described in terms of
avoiding excessive dorsi-flexion and foot "slam down"], thus
giving a softer landing(4)".
The "softer landing" described above may well be so, but
peri-patella pain is often a symptom of excessive "Q" or Quadriceps angle.
Excessive "Q" angle is associated with "flat foot", and tibial medial rotation(13).
What is not generally recognised is that femoral medial rotation is also a
contributor to excessive "Q" angle, and that "engaging Gluteus maximus"
(which is a powerful lateral rotator of the femur) will help correct femoral medial rotation
and significantly reduce the Q angle and associated peripatella pain. That is a lot to take on board! -
The diagrams in the next section should make things clearer.
"Q" Angle defined:
The "Q" angle is the angle between a line drawn through the patella tendon and a line drawn through
the Rectus femoris (see picture to right). It should be less than 20 degrees in men and less than 25
degrees in women(13).
The "Q" angle is increased to potentially harmful levels when the femur rotates medially
and the foot arch collapses (see diagram). Standard medical
therapy involves taking comfortable
shoeing to yet another extreme, with custom orthotic to correct flat feet and support the "collapsed" foot arch,
and thereby combat the medial rotation of the tibia. This does work, but like many physical
and surgical support strategies will never be 100% successful without attention
to optimization of muscle function and body positioning.
A better answer is to "engage Gluteus maximus at heel strike", and to form the foot arches. The shoe inserts
(custom orthotics) should be a last resort.
|
Q angle measurement for a subject instructed to "relax the gluteals and let the
foot arch flatten". The angle is 24 degrees.

|
Q angle measurement for the same subject instructed to "tense the gluteals and
form the foot arch". The angle is 15 degrees.

|
|
Note: The subject above has "Pes anserinum bursitis" of his left knee. This is
associated with his excessive resting Q-angle.
Pain over the medial knee is the key symptom, and this has greatly reduced with the help of
"bare-foot" running sessions combined with "contracting Gluteus maximus at heel strike" throughout the day.
(See appendix "Pain Free Running in Just Three Months!").
|
6. Tensor Fascia Lata - Iliotibial Band (FTL-ITB) Strain and Trochanteric Bursitis
"Stressed ilio-tibial band syndrome ... [is] attributed
to excessive shock loading of the limbs. When running barefoot on
hard surfaces, the runner compensates for the lack of cushioning underfoot by
plantar-flexing the foot at contact [probably better described in terms of
avoiding excessive dorsi-flexion and foot "slam down"], thus
giving a softer landing(4)".
And the better Reason...
Bare-foot running does reduce the shock loading of the limb, but
a clinical anatomy book graphically portrays the better reason. In the picture to the right,
we see the Iliotibial band together with the muscles that tension it. 80% of the fibres of the
Gluteus maximus insert onto the Iliotibial band, or ITB (3). If the Gluteus maximus is none functional,
that leaves the Tensor fascia lata (TFL) and the tendinous portion of the ITB that originates
from the hip bone to take the abductor loading of single leg stance. When this huge
muscle is not contributing to the load sharing, it is small wonder that the remaining
portion of the TFL and ITB becomes strained!
|
|
Please note: if you are suffering from
TFL-ITB strain, or Trochanteric bursitis, do not immediately go overboard with Gluteal contraction!
A gradual approach is required, which incorporates improvement of the function of a number
of muscle groups together with correction of "hip adduction with medial rotation"
(already referred to in this article). The reader
is referred to the relevant case study in Professor Sahrmann's text(3), and some exercises are suggeted below.
Where to now?
In this article, you have learned the consequences of poor function of the gluteus maximus.
You may have some idea that your own lack of gluteal development is contributing to pain or dysfunction.
You may be wondering what you should do about it. The printable Pilates Exercise Instructions listed below
(and on the previous three pages)will
be a great place to start!
If you have any comment, queries or critique, please contact me!
Contact Author
Thank you for taking the time to read this article!
Here is wishing you the very best of "Bushman's buttocks"!!!!
Regards,
Bruce Thomson
P.S.
The key message from this online article:
The solution for 'Structural" leg Problems is a strong and functional Gluteus maximus,
alongside strong and functional foot arches and
Posture-Movement Optimization!
The following free pilates exercises were instrumental in "fixing" my lower back pain, and flat feet/plantar fasciitis.
As I have already stated, I have thrown away my custom orthotics, and you may be able to do the same - subject to the
advice of your health care professional.
I encourage you to print the following exercises off and put them into your daily routine!
-
The Monkey (Gluteus maximus workout).
The Runners Squat (Gluteus maximus workout).
Arching the Foot (flat feet arch exercise)
Pointing and Flexing the Foot (flat feet/arch exercise)
Up and Down with a Tennis Ball(Composite exercise).
-
Have I helped you achieve your goal of freedom from "structural" leg pain?
Please make a donation!

Thank you!
Bruce Thomson
|
| P.S. Here are two web searches that I have found useful in my search for
Cures to my "structural" leg pain: - Perhaps they will help you too? - |
|
|
Return to top...
Engaging Gluteus Maximus and Minimizing Foot
and lower Leg Injuries
© Bruce Thomson, EasyVigour Project
|
Film Footage of Bushman Walking and Running!
Two classic low budget comedies from the 80's.
The first disc has a documentary feature on the real life of star
N!xau who played Xixo.
"If you're willing to laugh at
yourself, pick these up!"
(Mark Baker, Amazon.com review)
|
|
|
